
Key pharmacological differences between side effects of refined, pharmaceutical CBD formulations and whole plant extracts:
By: Mike Robinson (The former authors have vacated their positions due to 'controversy' over the subject matter / Edited 10/24/2018)
DRAFT
Abstract: (This is not the final draft, the final will be transformed into a more scientific document by a team in the following weeks)
Recent studies on the effectiveness of cannabidiol in the rare seizure disorders Dravet Syndrome and Lennox-Gastaut syndrome have prompted a biopharmaceutical company to perform clinical trials of its own to bring a cannabidiol-based drug to the American market through the process of FDA approval. Side effects were very prevalent in 79% of all patients taking a refined CBD product, some of which were severe like thrombocytopenia and transaminase elevations in the liver. However, there are indications from studies done with cannabidiol-rich cannabis extracts in Israel that indicate that fewer side effects (46%) are achieved with a natural cannabis plant extract containing a 20:1 ratio of CBD to THC. This paper seeks to answer why refined cannabinoids have more side effects than the natural cannabis product, as well as the possible etiology of said adverse reactions. Also discussed are other attempts at affecting the cannabinoid system from a singular standpoint. Ultimately, the cannabinoid system works by way of multiple molecules affecting multiple receptors at once – the entourage effect, and thus such singular approaches to treatment by way of the cannabinoid system are not effective. Traditional plant extracts contain many compounds in addition to THC and CBD that contribute to the medical benefits of cannabis.
Introduction:
Recently, a formulation of cannabidiol was approved by the United States FDA. It is extracted from hemp grown using conventional agricultural methods like pesticides and fertilizers and extracted using supercritical carbon dioxide, crystallized, and put into a formulation with sesame oil, strawberry flavoring, alcohol, and sucralose, to be used alongside existing anti-seizure medications like clobazam. This differs sharply from the conventional course of cannabis medicine, which is to use whole, clean plant extracts to treat epilepsy and to gradually discontinue the use of conventional pharmaceuticals. The question is, is there truly a difference? It might be argued by some that a compound is a compound, carbon for carbon, and thus it would have the same effects. However, it is sometimes the case that the pill binder or other carrier causes a medication issue. A review of the research must be done to find if natural plant extracts have an advantage over synthetic delivery systems.
Review:
During an open-label trial of pure CBD with Lennox-Gastaut and Dravet patients, 79% of all patients reported side effects. The most common side effects reported were somnolence (25%), decreased appetite (19%) diarrhea, (19%) Fatigue, (13%) Elevated liver enzymes, (7%) Convulsion, (11%) Increased appetite, (9%) Status epilepticus, (8%) Lethargy, (7%) Weight increased, (7%) Weight decreased, (6%) Drug concentration increased, (6%). Serious side effects in 30% of patients included status epilepticus in 6%, severe hepatotoxicity in 1 patient, and hyperammonemia in another. One patient died but it was ruled to be part of the course of their disorder and not a drug effect. The liver and urea cycle side effects were related to the co-intake of valproate, the pre-existing medication. (1) The official FDA side effects include insomnia (11%) irritability (9%), a chance of suicidal ideation “common to anticonvulsants” and a 33% higher chance of infection. It makes no mention of any interaction with valproate (2) CBD was also found to increase the active metabolite of clobazam, a common medication for refractory epilepsy, by blocking cytochrome p450 enzymes CYP2c19 and 3A4. (3) All side effects were for a 70% overall seizure reduction and 52% reporting a decrease of 50% or more.
An Israeli study of cannabis versus epilepsy, however, used natural extracts with a ratio of 20:1 CBD:THC. When administered to children with epilepsy, seizure reduction occurred in 89% of patients, and 54% achieved over 50% reduction. Only 7% had an increase in seizures, and only 7% had restlessness and irritability. 34/74 patients in all had side effects or 46%. (4) Interestingly enough, Aran noted a similar prevalence of irritability and restlessness in the Israeli CBD trial for autism, further underlining the connections between autism and seizures. (5). In all of these trials, none of the patients were on other medications concurrently – it is common practice in cannabis medicine in both California and Israel to withdraw from other medication. No hepatic side effects were noted.
These two studies are not alone in their findings. A recent meta-analysis of CBD studies on Dravet, Lennox-Gastaut, and CDKL5, 5 of them using purified CBD and 6 of them using a CBD-rich extract, found more improvement in general with CBD-rich extracts. However, the number of patients experiencing a reduction of 50% or more held steady between the two groups at 39-42%. The CBD-rich extract group had a lower effective dose on average, 6.1 mg/kg while purified CBD required 27.1 mg/kg. Purified CBD also tripled the rate of both mild side effects such as appetite alteration, sleepiness, gastrointestinal disturbances/diarrhea, weight changes, fatigue, nausea, and severe side effects such as thrombocytopenia, respiratory infections, and alteration of liver enzymes. (6)
Discussion:
There are two possible explanations for the reduced side effect profile and increased efficacy of the whole plant extracts versus the refined CBD product now on the market. One of the main things that stand out is that in America, CBD was investigated as an adjunct to existing AEDs while in established cannabinoid medicine, patients are gradually withdrawn from existing drugs to use CBD. Drug interactions involving the liver are more common with multiple medications, and this is what was shown in the Lancet study. (1) Another is that the Israelis and others used whole plant extract with a small amount of THC in a 20:1 ratio. There is a phenomenon known as the “entourage effect” where the action of multiple cannabinoids and other plant compounds known as terpenes exhibit effects at a variety of receptors. This mimics what the endogenous cannabinoids do: they are synthesized at the same time in precise ratios, on-demand, to exert precise effects on receptors. A neutral carrier made of sesame oil, strawberry flavoring, and sucralose has no synergy with CBD whatsoever. (7,8) Meanwhile, the terpene linalool has been shown to decrease glutamate binding and limonene and caryophyllene together have been shown to limit hippocampal excitability. (9,10)
Sucralose is common to use in a pediatric formulation. Although regarded as safe by the FDA, sucralose has since been find to alter glucose uptake and hormonal response to glucose, including of course insulin, and cause obesity in rats. (11) This effect is controversial in humans: some studies have shown no effect on glucose absorption in acute administration of sucralose in humans. (12) However, increased absorption of glucose was found, with corresponding increased insulin levels and decreased insulin sensitivity. (13) The strawberry flavoring ethyl methylphenylglycidate is another component with more questions than answers. It is registered as a pesticide ingredient with the EPA, and in the filing, LD50 numbers in rodents are noted and teratogenicity was noted in chickens. (14) NIH Toxnet cites studies that say that at 10000 ppm in rat feed caused growth retardation and testicular atrophy, while at 5000 ppm caused the demyelination of the sciatic nerve and can provoke hypersensitivity reactions with chronic exposure. (15) But more directly, there were two cases noted where strawberry flavoring caused reflex seizures with initial gamma band activity in the anterior inferior insula, with decreased activity in the hippocampus. (16) This is of interest because CB1 receptors are connected to gamma band activity and are most active in the hippocampus. (17,18) Meanwhile natural cannabinoids and terpenes are metabolized normally, with possible positive effects on blood sugar and metabolism and no added risk of seizures. (19)
There have been other attempts to use a singular compound to affect the endocannabinoid system. For several years Dr. Piomelli at UC Irvine and his lab were involved in the development of FAAH inhibitors – substances that inhibited the breakdown of endocannabinoids. (20) The aim was to increase the level of 2-AG and anandamide in general so as to produce effective relief for a cannabinoid deficiency without any psychoactive side effects. Things seemed to go well in animal trials using URB597. (21) However, human trials of a similar compound BIA-10-2474 in France ended in disaster causing brain damage. (22) The problem in this case may have been off target inhibition of lipid metabolism in the brain, causing something similar to Tay-Sachs disease. (23) Piomelli predicted this might happen and he and other scientists disagree with how the French company went ahead with human trials. (24) Another famous attempt is the CB1 antagonist rimonabant – it was briefly tried as an appetite suppressant before it was found to cause anxiety, depression, and suicidal thoughts, causing Europe to ban the drug and major drug companies to stop researching the whole class of drug for human use. (25) Synthetic CB agonists, created to study the cannabinoid system, escaped the lab and became a whole new drug problem in the form of “Spice”. These chemicals have caused deaths and overdoses nationwide, causing New York to ban them on September 13, 2012 and the USA to follow suit, though new compounds are made every day. (26)
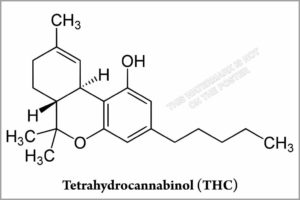
Another example of cannabinoid mono therapy is the THC pharmaceutical Marinol. After Professor Raphael Mechoulams discovery of THC as the main active principle in 1964, it took 22 more years for the FDA to approve its use as an appetite stimulant for AIDS and cancer patients, and only when all else had failed. (27) A 1998 study found a low potential for abuse and no indication of patients chasing the drug. (28) Side effects noted included strangely enough, vomiting and abdominal pain, psychiatric side effects including depression and paranoia, and low blood pressure. It has the same onset time of 60-90 min as cannabis edibles but only lasts 2-4 hours: many patients report edible cannabis made using the whole plant lasting 6-8 hours or more and find Marinol to be an inferior product (29,30). Concerns about mental and developmental health have been raised over THC and high THC cannabis concentrates, however CBD has been shown to moderate or even cancel out the effects of THC. (7). Hemp extracts are known to contain a small amount of THC even when derived from a CBD-rich cannabis cultivar and are known to produce positive test results for THC even in users of CBD hemp products. (31) The United States DEA has stated that small amounts of other cannabinoids will also occur in all cannabis extracts, even those that purport to be CBD only – unless synthesized de novo, CBD isolate will always contain small amounts of THC when extracted from a plant. Even chromatography is not perfect. If so, CBD medicines should warn of this at least for the purposes of drug testing. (32)
But how exactly does CBD by itself produce adverse effects in a small percentage of seizure and autism patients when it is well tolerated by 90% of the patient population? Even whole plant extracts are not tolerated by this group. This is where emerging science may provide an answer. CBD is mostly antagonistic towards the CB1 and CB2 receptors, with a Ki of 3500-4000 nanomolar. (33) It has been found to be a negative allosteric modulator of both of them. (34, 35) It is also an antagonist at GPR55 and 18 which have been shown to be secondary cannabinoid receptors (36,37). THC, for example, is a full agonist at GPR18. (38). Mutations in MBOAT7, which produces the natural ligand lycophosphatidylinositol for GPR55, are linked to autism. (39) A duplication of the region containing GPR18 was linked to another case. (40) It is thus possible that autism and seizure cases exist where the proper rescue pathway is through stimulation of the GPR receptors and not via the multiple, mostly antagonistic actions that CBD is known for. CBD and other cannabinoids are also known for having a bell-shaped dose-response curve. In an experiment with mice using CBD-rich extract, the anti-inflammatory and pain relief effects peaked at only 5 mg/kg, which is close to the average dose found in CBD-rich extract studies. However, the use of whole plant extract was able to overcome this and make the relationship correlative. It is possible that the dose used in studies using isolated CBD is too high in general and given the prospective study design in those studies versus the retrospective design used in the extract studies this remains a possibility. (41,6)
Conclusion:
Ultimately cannabinoid medicine must be based on a sound understanding of the underlying biological systems involved, as well as the unique human physiological response to inert synthetic ingredients that are proven herein to be the causation of most, if not all the side effects listed by the F.D.A. on the new pharmaceutical, and that the vast majority of these side effects are not from an extract of Cannabis, including CBD. As well, the conventional approach of isolating a single active principle and using it when a prior study does not support such applications within the Endocannabinoid System, where multiple components are manufactured by the same enzymes in ratios to exert an effect in concert on the system in a whole. More research is needed to determine proper ratios for specific conditions, as well as genetic testing developed to determine the appropriate course of treatment. In all, neither CBD nor THC alone are as opportune as monotherapy without other accompanying elements of the plant including phytocannabinoids and terpenes. Efficacy in a study is reduced when one cannabinoid is isolated away from the balance of the cannabis plant. The side effects stemming from the addition of synthetic inert ingredients to sweeten and flavor are found to be a risk of consideration for further study. When combined with other pharmaceutical medications, specifically seizure medications, the side effects are unnecessary and again, in a large part a cause of inert ingredients. In conclusion, the removal of Cannabidiol from its accompanying plant terpenes and other cannabinoids and its placement into a carrier consisting of sucralose, a synthetic strawberry flavoring, and sesame oil also reduces the effectiveness and heavily contributes to the F.D.A. listed common and severe side effects. There is no way to conclude that the new pharmaceutical compares to whole-plant extract in any scientific way other than containing an isolated cannabinoid. Regarding the warning for specific populations that are based on animal data, the pharmaceutical may cause fetal harm. There is sufficient data, as indicated in the discussion, that inert ingredients within this newly approved CBD pharmaceutical for the US Market have already been proven to cause harm in the unborn fetus and not the cannabinoid. This would explain the special warning upon the current FDA-approved drug. Moreover, since CBD can never be fully isolated, the packaging of CBD medicines should warn about the presence of THC.
References
- 1. Orrin Devinsky*, Eric Marsh*, Daniel Friedman*, Elizabeth Thiele, Linda Laux, Joseph Sullivan, Ian Miller, Robert Flamini, Angus Wilfong, Francis Filloux, Matthew Wong, Nicole Tilton, Patricia Bruno, Judith Bluvstein, Julie Hedlund, Rebecca Kamens, Jane Maclean, Srishti Nangia, Nilika Shah Singhal, Carey A Wilson, Anup Patel, Maria Roberta Cilio. Cannabidiol in patients with treatment-resistant epilepsy: an open-label interventional trial. Lancet Neurol Dec 23 2015.
- 2. FDA Epidiolex side effects warning sheet, revised
- 3. 1Alexandra L. Geffrey, 1Sarah F. Pollack, Patricia L. Bruno, and Elizabeth A. Thiele. Drug–drug interaction between clobazam and cannabidiol in children with refractory epilepsy. Epilepsia, 56(8):1246–1251, 2015
- 4. Moran Hausman-Kedem MD and Uri Kramer MD. Efficacy of Medical Cannabis for Treating Refractory Epilepsy in Children and Adolescents, with Emphasis on the Israel Experience. IMAJ, FEBRUARY 2017
- 5. ADI ARAN, Hanoch Cassuto, Asael Lubotzky. Cannabidiol Based Medical Cannabis in Children with Autism- a Retrospective Feasibility Study. Neurology, April 10, 2018; 90 (15 Supplement)
- 6. Fabricio A. Pamplona1*, Lorenzo Rolim da Silva2 and Ana Carolina Coan3Potential Clinical Benefits of CBD-Rich Cannabis Extracts Over Purified CBD in Treatment-Resistant Epilepsy: Observational DataMeta-analysis. Neurol. 9:759.
- 7. W-SV Ho1, DA Barrett2 and MD Randall1. ‘Entourage’ effects of N-palmitoylethanolamide and N-oleoylethanolamide on vasorelaxation to anandamide occur through TRPV1 receptors. British Journal of Pharmacology (2008) 155, 837–846
- 8. Ethan Russo. A tale of two cannabinoids: The therapeutic rationale for combining tetrahydrocannabinol and cannabidiol. Medical Hypotheses (18 aug 2005)
- 9. Ahmad Abdulla 1 , Mahshid Hosseini-Zareh 1 , Jok?bas Žiburkus. Cannabis terpenes synergistically modulate hippocampal excitability. Department of Biology and Biochemistry, University of Houston, Houston, TX.
- 10. Elisabetsky E1, Brum LF, Souza DO. Anticonvulsant properties of linalool in glutamate-related seizure models. Phytomedicine. 1999 May;6(2):107-13.
- 11. Kimihiko Mitsutomi, Takayuki Masaki?, Takanobu Shimasaki, Koro Gotoh, Seiichi Chiba, Tetsuya Kakuma, Hirotaka Shibata. Effects of a nonnutritive sweetener on body adiposity and energy metabolism in mice with diet-induced obesity. METABOLISM CLINICAL AND EXPERIMENTAL 63 (2014) 69 – 7 8
- 12. Jing Ma1,2, Jessica Chang3 , Helen L. Checklin1,2, Richard L. Young1,2,4, Karen L. Jones1,2, Michael Horowitz1,2,3 and Christopher K. Rayner1 .Effect of the artificial sweetener, sucralose, on small intestinal glucose absorption in healthy human subjects. British Journal of Nutrition (2010), 104, 803–806
- 13. YANINA PEPINO, PHD COURTNEY D. TIEMANN, MPH, MS, RD BRUCE W. PATTERSON, PHD BURTON M. WICE, PHD and SAMUEL KLEIN, MD. Sucralose Affects Glycemic and Hormonal Responses to an Oral Glucose Load. Diabetes Care. 2013 Sep;36(9):2530-5
- 14.http://pmep.cce.cornell.edu/profiles/miscpesticides/misc_E_N/ethyl_methylphen/ethmeth_pet_1200.html
- 15.https://toxnet.nlm.nih.gov/cgi-bin/sis/search/a?dbs+hsdb:@term+@DOCNO+1150
- 16. Blauwblomme T, Kahane P, Minotti L, et al Multimodal imaging reveals the role of γ activity in eating-reflex seizures Journal of Neurology, Neurosurgery & Psychiatry 2011;82:1171-1173.
- 17. Jose Cortes-Briones1,2, Patrick D Skosnik1,2,3, Daniel Mathalon2,4,5, John Cahill1,2,3, Brian Pittman2,3, Ashley Williams1,3, R Andrew Sewell1,2,3, Mohini Ranganathan1,2,3, Brian Roach4,5, Judith Ford2,4,5 and Deepak Cyril D’Souza*,1,2,3. Δ9-THC Disrupts Gamma (γ)-Band Neural Oscillations in Humans. Neuropsychopharmacology (2015) 40, 2124–2134
- 18. Davies SN1, Pertwee RG, Riedel G.Functions of cannabinoid receptors in the hippocampus.Neuropharmacology.. 2002 Jun;42(8):993-1007.
- 19. Pablo Juan-Pico´ a, Esther Fuentes a, F. Javier Bermudez-Silva ´ b, F. Javier D´?az-Molina b, Cristina Ripoll a, Fernando Rodr´?guez de Fonseca, Angel Nadal Cannabinoid receptors regulate Ca2+ signals and insulin secretion in pancreatic #Beta cell. Cell Calcium 39 (2006) 155–162
- 20. Darren Fegley, Silvana Gaetani, Andrea Duranti, Andrea Tontini, Marco Mor,Giorgio Tarzia, and Daniele PiomelliCharacterization of the Fatty Acid Amide Hydrolase Inhibitor Cyclohexyl Carbamic Acid 3 -Carbamoyl-biphenyl-3-yl Ester (URB597): Effects on Anandamide and Oleoylethanolamide Deactivation. JPET 313:352–358, 2005
- 21. Roberto Russo, Jesse LoVerme, Giovanna La Rana, Timothy R. Compton, Jeff Parrott, Andrea Duranti, Andrea Tontini, Marco Mor, Giorgio Tarzia, Antonio Calignano, and Daniele Piomelli The Fatty Acid Amide Hydrolase Inhibitor URB597 (Cyclohexylcarbamic Acid 3 -Carbamoylbiphenyl-3-yl Ester) Reduces Neuropathic Pain after Oral Administration in Mice. JPET 322:236–242, 2007
- 22. Christophe Mallet1,2, Claude Dubray1,2,3, and Christian Dualé1,3 FAAH inhibitors in the limelight, but regrettably. International Journal of Clinical Pharmacology and Therapeutics, Vol. 54 – No. 7/2016 (498-501)
- 23. Annelot C. M. van Esbroeck,1 * Antonius P. A. Janssen,1 * Armand B. Cognetta III,2 et al. Activity-based protein profiling reveals off-target proteins of the FAAH inhibitor BIA 10-2474. Science 356, 1084–1087 (2017)
- 24. New clues to why a French drug trial went horribly wrong. Science, June 2017
- 25. Bernard Le Foll, MD, PhD1, David A. Gorelick, MD, PhD2, and Steven R. Goldberg, PhD3. The future of endocannabinoid-oriented clinical research after CB1 antagonists. Psychopharmacology (Berl). 2009 July ; 205(1): 171–174.
- 26: http://rules.cityofnewyork.us/tags/synthetic-cannabinoids-10
- 27: Gaoni and R. Mechoulam. Isolation, Structure, and Partial Synthesis of an Active Constituent of Hashish. Journal of the American Chemical Society 1964 86 (8), 1646-1647
- 28: Calhoun SR, Galloway GP, Smith DE . Abuse potential of dronabinol (Marinol)”. Journal of Psychoactive Drugs. 30 (2): 187–96.(1998)
- 29: US Food and Drug Administration “Marinol (Dronabinol)” (PDF). September 2004.
- 30: “Cannabis effects by Erowid” https://erowid.org/plants/cannabis/cannabis_effects.shtml
- 31: Gero Leson et al. Evaluating the Impact of Hemp Food Consumption on Workplace Drug Tests. Journal of Analytical Toxicology, Vol. 25, November/December 2001
- 32: United States DEA. Establishment of a New Drug Code for Marihuana Extract. https://www.deadiversion.usdoj.gov/fed_regs/rules/2016/fr1214.htm
- 33: RG Pertwee. The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: D9 -tetrahydrocannabinol, cannabidiol and D9 -tetrahydrocannabivarin. British Journal of Pharmacology (2008) 153, 199–215
- 34: R B Laprairie1 , A M Bagher1 , M E M Kelly1,2 and E M Denovan-Wright1. Cannabidiol is a negative allosteric modulator of the cannabinoid CB1 receptor. British Journal of Pharmacology (2015) 172 4790–4805
- 35: Eva Martínez-Pinilla1 * † , Katia Varani2† , Irene Reyes-Resina3,4† , Edgar Angelats3,4 , Fabrizio Vincenzi2 , Carlos Ferreiro-Vera5 , Julen Oyarzabal6 , Enric I. Canela3,4 , José L. Lanciego7 , Xavier Nadal5 , Gemma Navarro3,4,8 , Pier Andrea Borea2 and Rafael Franco. Binding and Signaling Studies Disclose a Potential Allosteric Site for Cannabidiol in Cannabinoid CB2 Receptors. Front. Pharmacol., 23 October 2017.
- 36: McHugh, D., Hu, S. S., Rimmerman, N., Juknat, A., Vogel, Z., Walker, J. M., et al. (2010). N-arachidonoyl glycine, an abundant endogenous lipid, potently drives directed cellular migration through GPR18, the putative abnormal cannabidiol receptor. BMC Neurosci. 11:44.
- 37: Ryberg, E., Larsson, N., Sjögren, S., Hjorth, S., Hermansson, N. O., Leonova, J., et al. (2007). The orphan receptor GPR55 is a novel cannabinoid receptor. Br. J. Pharmacol. 152, 1092–1101.
- 38: Douglas McHugh1 , Jeremy Page1 , Emily Dunn1 and Heather B Bradshaw. D9 -Tetrahydrocannabinol and N-arachidonyl glycine are full agonists at GPR18 receptors and induce migration in human endometrial HEC-1B cells. British Journal of Pharmacology (2012) 165 2414–2424
- 39. Anide Johansen,1,2 Rasim O. Rosti,1 Damir Musaev,1 Evan Sticca,3 Ricardo Harripaul,4 Maha Zaki,5 Ahmet Okay C¸ aglayan,6 Matloob Azam,7 Tipu Sultan,8 Tawfiq Froukh,9 Andre´ Reis,10 Bernt Popp,10 Iltaf Ahmed,11 Peter John,11 Muhammad Ayub,12 Tawfeg Ben-Omran,13,14 John B. Vincent,4 Joseph G. Gleeson,1,3,15,* and Rami Abou Jamra10,16. Mutations in MBOAT7, Encoding Lysophosphatidylinositol Acyltransferase I, Lead to Intellectual Disability Accompanied by Epilepsy and Autistic Features. The American Journal of Human Genetics 99, 912–916, October 6, 2016.
- 40. Atack a H. Fairtlough b K. Smith a M. Balasubramanian. A Novel (Paternally Inherited) Duplication 13q31.3q32.3 in a 12-Year-Old Patient with Facial Dysmorphism and Developmental Delay. Mol Syndromol 2014;5:245–250.
- 41. Gallily, R., Yekhtin, Z. and Hanuš, L.O. (2015) Overcoming the Bell‐Shaped Dose‐Response of Can‐ nabidiol by Using Cannabis Extract Enriched in Cannabidiol. Pharmacology & Pharmacy, 6, 75‐85.
A Note from Mike:
As a patient with severe epilepsy and a father of not one but two children with it? I will let the research and study we have done speak for itself for the most part, but I’ll be backing it with public appearances and interviews to head off the ‘side effect’ warnings that we WILL SEE on TV and hear on the radio. This is serious – CBD is under attack and by the use of a very disturbing way of creating a product for children. The topic of inert ingredients in CBD products has been ongoing since the inception of the many different types of oils we see on the market. Never have I personally witnessed anything quite like this. My opinion on this all will come in a future blog, at this time we’re doing initial publishing as there are multiple entities, mostly Epilepsy Societies and Foundations, that are awaiting this document for analysis and publication.

This is what good full extract CBD oil can look like, you will not find this on a pharmaceutical store shelf nor will you find via a prescription by your doctor who likely knows very little, if anything, about Cannabis.

Full Spectrum CBD products of the best type, many times will come from the same type of Cannabis flower or bud that the THC crowd loves. Genetics have allowed Cannabis to advance quickly.
There’s simply no excuse for bastardizing the plant in a manner we see here in the extremely factual and well-planned research study above. Over 50 well-known researchers globally weighed in, and many with varying opinions. But the facts that James and I initiated seemed to be the ones that most are paying attention to. Inert ingredients coupled with a single cannabinoid delivery created through an odd lab process create a product that fails to meet efficacy standards and meets all nonstandards of causing side effects that include increased seizures. This makes no sense unless the plot in releasing this drug that will only serve 1/2 of 1% of the world of Epilepsy was to once again marginalize cannabis by using already marginalized people like myself – those with Epilepsy. Those the world writes off for the most part anyway.
The inert ingredients within the newly approved Pharmaceutical CBD are not only in a large way responsible for key very concerning side effects within it but are known to promote seizures in a big way – proven with studies on the exact same flavoring. Why would a pharmaceutical company do this? But it gets worse, these are carcinogens and are blatantly unsafe in my strong professional opinion.
The fact that this ‘CBD only’ pharmaceutical can cause a positive THC test per the DEA rule 7350 yet has NO WARNING? Now that seems beyond dangerous to consumers – it’s downright irresponsible on both the pharmaceutical companies’ behalf and the FDA/DEA combo who seem to not read each other interoffice memos.
Thank you,
Mike Robinson, Medicinal Cannabis Patient & Director of Consumer Affairs, American Academy of Cannabinoid Medicine, Founder, Research Institute

Sign up to receive informative and exciting email updates from Mike's Medicines!
You can sign up for our mail list here:
Didn't find what you are looking for?
Find exactly what you want to when you want it.
Browse through our archives by date, category or by entering a topic in the provided search field.
Archives
Categories
More to come as we have time to add them – there’s 100’s of additional publications!

We’ve made it easy for you to read Mike’s Medicine Blog or visit any of the Menu items right from here. It is that simple! Explore Mikes Medicines by clicking on the button below:


Read about how Cannabis Compassion and love created Mike’s beautiful family, the Cannabis Love Story inspires millions daily:

Genevieve’s Dream is all about her love for the Carousel coupled with her Cannabinoid Medicine journey – read more and make contact if you’re interested in collaborating with Mike!

The Global Cannabinoid Research Center is a trusted source for education, R&D, and more – make contact with us to collaborate.
Global Cannabinoid Research Center

